info@helpwithnursingassignments.co.uk
info@helpwithnursingassignments.co.uk 
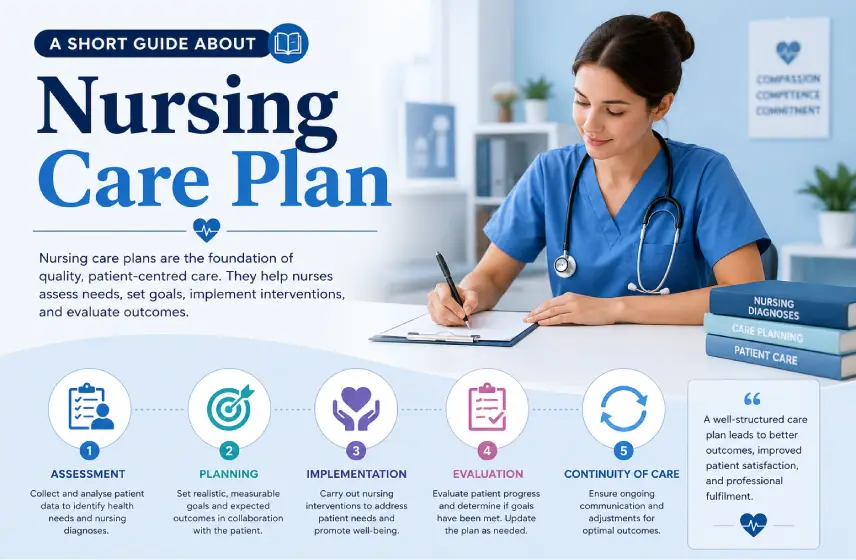
In every healthcare setting, including hospitals, clinics, rehabilitation centers, and home care, nurses play an essential role in providing effective, patient-centered care. Furthermore, one of the most crucial tools they use is the nursing treatment plan.
Think of it as more than just a checklist. It is like a structured roadmap that shows patient needs, sets goals, plans interventions, and evaluates outcomes.
It makes sure that every action is purposeful, evidence-based, and aligned with the patient's unique condition. Whether you are a nursing student, an early career nurse, or someone simply wanting to understand how modern healthcare works, knowing the vital points of a nursing treatment plan is essential. In this blog, we will dive deep into every part of a nursing treatment plan, what it includes, why it matters, and how it improves patient outcomes.
What Is a Nursing Treatment Plan?
A nursing treatment plan is a formal document showcasing the care the patient requires based on a comprehensive assessment. Furthermore, unlike generic medical plans, these nursing plans emphasize holistic care, considering not only physical health but also emotional, psychological, social, cultural, and spiritual needs. Furthermore, its purpose is to:
-
Organize and prioritize patient care
-
Furthermore, guide nurses in their daily responsibilities
-
Moreover, promote consistency across shifts
-
You also need to ensure patient safety
-
Also, you have to provide measurable outcomes
-
It even enhances communication among healthcare teams
-
This also helps in improving patient satisfaction and recovery.
Well, the nursing treatment plans are dynamic. Furthermore, it changes as the patient progresses, responding to the treatment or developing new needs.
Why Are Nursing Treatment Plans Important?
When it comes to the nursing treatment plans, they serve several critical functions. They include:
-
Ensuring Patient-Centered Care: Every plan is tailored to the patient based on their diagnosis, lifestyle, preferences, and risks.
-
Improves Communication Among Healthcare Providers: Doctors, nurses, therapists, and caregivers can all refer to the same plan to stay coordinated.
-
Enhancing Clinical Judgement: Creating NCP Example and plans push nurses to think critically, assessing patient data, analyzing patterns, and determining the best course of action.
-
It Measures Outcomes and Adjusts Care: Moreover, the clear goals allow nurses to track what is working and what needs modification.
-
Supporting Legal and Ethical Practice: Documentation protects both patients and professionals. Thus, this ensures transparency and accountability.
Core Components of a Nursing Treatment Plan
When it comes to creating nursing treatment plans, there are some core components. However, the formats may vary slightly across hospitals and educational institutions. Come on! Here is the in-depth explanation of nursing care plan writing help examples. Come on! Have a look at them.
-
Patient Assessment
The nursing process always begins with assessment. Thus, this involves collecting comprehensive, accurate data about the patient’s condition. Here is the in-depth detail:
Types of Data Collected
There are different types of data collected, which include:
Subjective Data
It is what the patient says. For example:
-
I feel pain in my lower abdomen.
-
I haven’t eaten well for several days.
-
I’m feeling anxious about surgery.
Objective Data
This type of data usually includes what the nurse observes or measures.
For example:
-
Vital signs, which include heart rate, blood pressure, and oxygen saturation
-
Lab results
-
Physical exam findings
-
Observed behavior or symptoms
Holistic Assessment Includes:
It is mostly what you feel. For example:
-
Physical health
-
Emotional and psychological status
-
Social and family background
-
Cultural and religious considerations
-
Functional ability (mobility, ADLs)
-
Risk factors (falls, infections, pressure injuries)
Moreover, the accurate assessment is the foundation of a meaningful treatment plan. Furthermore, without it, the rest of the plan loses its direction.
Nursing Diagnosis
Once assessment data is collected, nurses use standardized terminology, which is often known as NANDA-I (North American Nursing Diagnosis Association International). The main purpose is to identify a nursing diagnosis.
However, do remember that the nursing diagnosis is different from a medical diagnosis. Come on! Let’s learn the main difference between them.
Medical Diagnosis:
This is a diagnosis identified by a physician, for e.g., pneumonia, diabetes, or fracture.
Nursing Diagnosis:
This is the diagnosis identified by patient responses to the medical condition. For e.g., impaired gas exchange, acute pain, risk for infection. There are different types of nursing diagnoses that you should know about. They include:
Types of Nursing Diagnoses
-
The first one is the Problem-Focused Diagnosis, which focuses on a current issue that is supported by the evidence. For example, it could be the acute pain related to a surgical incision as evidenced by verbal complaints of pain.
-
The second is the risk diagnosis, which shows the potential issue that may occur. For example, it could include the risk for falls related to unsteady gait.
-
Another common example is the Health Promotion Diagnosis. It talks about the patient’s readiness for their well-being. For example, it could be how a patient enhances their nutrition.
Remember, each diagnosis must be backed by the assessment evidence. Furthermore, clear diagnoses help nurses select the best interventions. To learn more about this, you can consider checking out the nursing care plan template.
Setting SMART Goals and Expected Outcomes
Here comes the third step! Now you need to transform the diagnosis into measurable objectives. So what are the SMART Goals? Let’s find out.
What Are SMART Goals?
They are:
-
Specific
-
Measurable
-
Achievable
-
Relevant
-
Time-bound
Examples of SMART Goals in Nursing
To help you understand what SMART Goals look like, here are some examples for you:
-
Patients will report pain levels decreased to 3/10 within 24 hours.
-
Additionally, the patient's oxygen saturation will remain above 95% during the shift.
-
Moreover, patients will demonstrate proper insulin self-administration before discharge.
What’s the Difference Between the Short-Term vs. Long-Term Goals?
Let’s understand the difference between the Short-Term and Long-Term Goals. They include:
-
Short-term goals: They are usually achievable within hours or days. For example, it could be stabilizing vital signs.
-
Long-term goals: These types of goals usually focus on rehabilitation or lifestyle improvement. For example, regaining stability after the stroke.
Always remember that clear goals guide the entire treatment plan. Furthermore, it also helps you track progress.
Nursing Interventions
These nursing interventions are the actions nurses take to achieve the expected outcomes. They may be independent, dependent, or collaborative. Furthermore, there are different types of nursing interventions that you need to know.
Types of Nursing Interventions
-
Independent Interventions
Think of it as the actions a nurse can perform without a physician’s order. For example,
-
Teaching deep breathing exercises
-
Furthermore, repositioning the patient to prevent pressure ulcers
-
Also, it monitors vital signs
-
Furthermore, they also provide emotional support
-
Dependent Interventions
Furthermore, in these interventions, actions require the physician's approval. For example:
-
Checking the prescribed medicine.
-
Furthermore, implementing a wound care regimen ordered by a doctor.
-
Starting oxygen therapy.
-
Collaborative Interventions
It is performed with other healthcare professionals. For example:
-
Working with physical therapists on mobility programs
-
Additionally, coordinating dietary plans with nutritionists
-
Collaborating with social workers for discharge planning
Examples of Interventions per Diagnosis
Diagnosis: Acute Pain
Interventions may include:
-
Assess pain every 4 hours
-
Administer analgesics as prescribed
-
Apply heat or cold packs
-
Teach relaxation techniques
Diagnosis: Risk for Infection
Interventions may include:
-
Maintain sterile technique
-
Monitor wound drainage
-
Educate the patient on hygiene practices.
Always make sure that the interventions are evidence-based and relevant to the patient’s condition.
Rationale for Each Intervention
When it comes to the nursing treatment plan, it also includes rationales.
But what are they?
Well, they are the explanations for why each intervention is necessary. Furthermoe, they connect theory to practice. Here is the example:
-
Intervention: Reposition the patient every 2 hours
-
Rationale: Reduces pressure on bony prominences and lowers the risk of pressure injury.
This shows that every action has a purpose. Furthermore, it helps students understand clinical decision-making.
Evaluation of Outcomes
Evaluating the nursing care practices determines if the goals were met. Furthermore, it has three possible conclusions, including:
-
Goal Met – It shows that the desired outcome has been achieved
-
Goal Partially Met – This shows some progress but the goals are not met.
-
Goal Not Met – No progress or the condition has worsened.
Now the question is what happens after the evaluation:
-
You should continue the existing plan if it is effective.
-
Modify interventions if progress is slow.
-
Furthermore, reassess the patient if the condition worsens.
-
Make sure to set the new goals.
-
Discontinue goals that have been achieved.
This keeps the plan dynamic and adaptable.
Documentation
In nursing care plans, accurate documentation is a professional and legal requirement. So the question is, what should be documented?
-
Patient assessment findings
-
Nursing diagnoses
-
Implemented interventions
-
Patient responses and progress
-
Any changes to the plan
-
Communication with other healthcare providers
-
Education given to the patient or family.
Furthermore, documentation ensures the continuity of care and protects both patients and nurses.
Conclusion
This brings us to the end of the guide! Understanding the components of nursing treatment plans is essential for delivering effective, structured, and holistic patient care. Each section, from assessment to evaluation, serves a specific purpose in guiding clinical decisions. Furthermore, it improves outcomes and ensures safe practice.
Additionally, nursing treatment plans are not static documents. Furthermore, they are living tools that evolve alongside the patient. Through these elements, nurses strengthen their critical thinking, enhance communication and elevate the overall quality.